Plain language summary (What is this?)
- Megan is a psychiatric survivor and Vicky lives in a long-term care facility. Together, we share our experiences of being violated, assaulted, and desexualized in health care institutions like psychiatric wards, hospitals, and long-term care facilities.
- We argue that sexual violence and controlling disabled people’s sexuality is foundational to these institutions. We share Canada’s history of sterilizing (making sure disabled people can’t have children), segregating (separating disabled and non-disabled people), and institutionalizing (locking up disabled people in institutions).
- We argue that disabled people have their own sexual culture. It teaches us that there are infinite possibilities to sex, beyond what we are taught sex should be: a straight man penetrating a straight woman.
- Institutions close the doors on those possibilities. Ending institutionalization is an important part of justice for all disabled people and all people who have sex.
Megan:
Locked in the psychiatric ward, a nurse removes me from my wheelchair and gestures for me to spread my feet. Legs shaking, a strip search begins. An older psychiatric nurse demands I remove every single piece of clothing, including my bra and underwear. Hands shaking, I comply. I know it’s finally over when the nurse issues me the standard psychiatric patient uniform: grippy psychiatric socks (no shoes, never shoes) and suicide pajamas – a single piece of cloth that fastens at the back with Velcro.
Instances of normalized violence in the psychiatric and medical system like this haunt the “care” I require to survive. In recent years, the Supreme Court recognized “that many, including women and minorities, experience strip searches as sexual assaults.” Despite this, I’m still strip-searched and my clothing is forcibly removed when I enter the hospital. Prison abolitionist and scholar Dean Spade puts the violence of prisons – and I do consider institutions akin to prisons – bluntly: “The prison is not a way to stop rape, the prison is the rapist.”
The only way I survive this system is with crip humour – cracking dark jokes with other disabled people about the ableist violence we’re forced to endure in order to survive. I met Vicky Levack doing just that – sharing stories about the state and interpersonal violence inflicted on us behind institutional walls.
Vicky and I tell our stories with a smile, but these stories should haunt you.
I’m a psychiatric survivor, patient, researcher, and creator of the Invisible Institutions podcast, which tells the stories of survivors of institutions for people labelled with intellectual and developmental disabilities in Canada. Vicky’s a resident of Arborstone Enhanced Care, a long-term care facility in Halifax. Like thousands of other disabled people in Canada, she didn’t choose to live in an institution – she was left with no other option. For over 10 years, the Nova Scotia government has refused her social assistance and at-home care services, forcing her to move into Arborstone at the age of 21.
Vicky and I tell our stories with a smile, but these stories should haunt you. We tell these deeply personal stories to disrupt the silence and invisibility created by institutional walls. We’re enraged by the normalization of locking up disabled people in institutions, as well as the violence and loss of autonomy residents endure. As a disabled woman and a disabled femme, our experiences with violence and loss of autonomy in institutions are sexualized and gendered.
We believe that these aren’t problems that can be reformed away – they’re the bedrock of why institutions were created in the first place. Together, we share our histories to unpack the violence foundational to disability institutions, along with crip resistance to confinement.
Vicky:
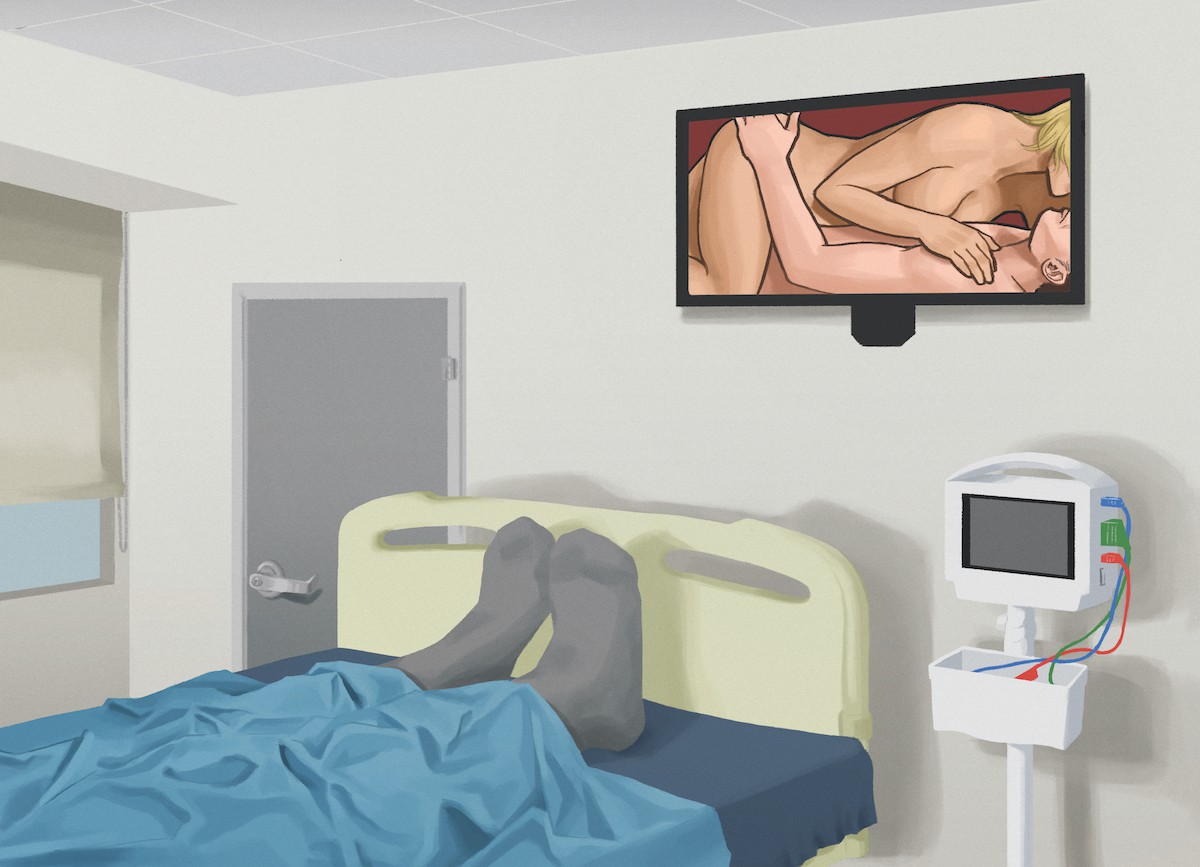
Locked in Arborstone during the first wave of the COVID-19 pandemic, I wanted to watch erotic movies.
I love porn. I subscribe to PassionFlix; they make erotic movies for women, and it’s all made by women and based on romance novels. I’m a romance novel junkie, so when I heard about this service, I was like, “Please shut up and take my money.”
One day, I told the nurses, “I’m going to watch this movie. Can you close my door please?” And they said, “Of course we can do that.”
In the film, there’s some simulated oral sex and of course right when I got to that part, a personal care attendant walked in.
We joked about it, we laughed. But that was a little awkward for me.
Living here, I have to prove that I’m an adult and that I’m a sexual being.
The surveillance and lack of privacy at Arborstone is infantilizing, and it prevents the institution from becoming a home where I can feel safe.
Living here, I have to prove that I’m an adult and that I’m a sexual being. I’ve fought for my right to fuck. The nurses told me that no one ever wanted to have sex here before I came, that it never came up.
Megan:
Institutions like long-term care facilities have a long history of inhibiting and controlling the sexual lives of the disabled people confined to them. Throughout the late 1800s, institutions for people labelled with mental disabilities were built across Canada. During this time, race science – which held that white, wealthy, non-disabled people were genetically superior – was popular, and it served an important role in justifying Canada’s genocidal settler colonialism and white supremacy. Eugenics was a critical component of this. The term was coined in 1883 by Sir Francis Galton, who defined it as “the science of improving stock,” not only by “judicious mating, but [whatever] tend[s...] to give the more suitable races or strains of blood a better chance of prevailing speedily over the less suitable.” While Galton was in England, eugenics proliferated globally through Eugenic Societies intending to eliminate not only racialized people but also people with disabilities.
Eugenics understood mental disabilities as infectious, hereditary, and in need of extinction. Prominent Canadian politician and eugenicist Nellie McClung summarized the ableism inherent to eugenics: “to bring children into the world, suffering from the handicaps caused by the ignorance, poverty, or criminality of the parents, is an appalling crime against the innocent and helpless, and yet one about which practically nothing is said.”
In 1928, Alberta passed the Sexual Sterilization Act, which resulted in the creation of the Alberta Eugenics Board, and a similar act was passed in British Columbia in 1933. The Alberta Eugenics Board subjected at least 2,834 people labelled with intellectual disabilities to involuntary sexual sterilization. This Act relied upon Alberta’s institutions for people labelled with mental disabilities – namely the Michener Centre – to identify candidates for sterilization, and carried out the sterilizations in their facilities.
But state-mandated eugenicist practices didn’t cease to exist – they were buried in the language of bureaucracy.
While the rest of the provinces didn’t have explicit sterilization policies, they controlled the sex lives of their residents through institutional design, by building institutions far outside of city limits and segregating patients by sex. As one Ontario government commissioner summarizes: “So keen were the officials that there be no possibility of sex or propagation by these deviants that upon death men and women were sometimes buried in separate burial grounds.”
After Nazi Germany’s extensive use of eugenics to kill Jews, queer people, racialized people, Roma, and disabled people, the term “eugenics” fell out of fashion in the 1950s and 1960s. But state-mandated eugenicist practices didn’t cease to exist – they were buried in the language of bureaucracy.
Since their inception, institutions have changed their names, from “asylums for idiots and the feebleminded” to “regional centres,” putting up different facades to maintain their relevance while continuing to practice eugenics. I’m from Winnipeg, writing in Ottawa, and Vicky is in Halifax. These three provinces we span – Manitoba, Ontario, and Nova Scotia – have unique stories of institutionalizing disabled people. In Manitoba and Nova Scotia, there are a number of large, segregated institutions for people with disabilities. The Selkirk Mental Health Centre in Manitoba is one of the largest remaining remote psychiatric institutions in Canada, and the government has no plan to close it. In Ontario, the last three institutions for people labelled with developmental disabilities closed in 2009. And in Nova Scotia, the government plans to close large institutions for people labelled with intellectual/developmental disabilities and move people into smaller institutions like small-option homes, but those plans continue to be delayed.
The culture of segregation and punishment not only limits disabled people’s access to their sexuality but puts them in harm’s way.
Today’s institutions, like Vicky’s nursing home and my psychiatric institution, remain the default housing and care option for disabled people, continuing the legacy of disability institutionalization. Even the designs of contemporary institutions are similar to early 20th-century ones: shared rooms to prohibit our access to our own sexuality, sex segregation, and non-stop surveillance by staff.
Most of the psychiatric wards I have been in are not sexually segregated, but prisons, forensic psychiatric wards, group homes, and many other forms of congregate housing are. Scholar Natalie Chin calls institutions and their policies “sex police,” with staff looming over the CCTV (the video surveillance system) and wandering into patient rooms where the doors don’t lock (but the front doors of the ward sure do). In psychiatric institutions and prisons, internet and phone access are highly controlled, preventing any opportunity for communication with the outside or, say, to watch porn. In many cases, acts of sexuality like masturbation and watching porn are pathologized and might be met with solitary confinement, isolation, or “lock-up”. The culture of segregation and punishment not only limits disabled people’s access to their sexuality but puts them in harm’s way.
Today’s institutions weren’t built with care in mind, but control. Institutional administration controls every aspect of residents’ lives, from what they eat to when they leave, to their access to privacy and sexuality. The lack of control residents have over their lives is framed as “care” by the institution and health care professionals, but it is rooted in a history of eugenics and puts residents at risk.
Vicky:
I should never have been in a system where I was made vulnerable. I’ve been subject to more harm and violence in this system than I would ever have been if I were living in the community.
I live on the first floor of Arborstone now, but when I lived on the second floor, I did not have a private room and that exposed me to violence. I was assaulted three times in that unit. I requested that I be moved to a private room in the other unit, but [Arborstone’s administration] refused. I had to go to the press to shame them into giving me a private room. I should not have had to go public. I should not have been assaulted once, twice, or three times.
Megan:
There is a high prevalence of sexual violence within and beyond institutions. This violence that Vicky and I have been exposed to is a part of the disability experience in Canada. Research shows that disabled women are four times more likely to have experienced sexual assault than non-disabled women.
In The Sexual Politics of Disability: Untold Desires, disability scholars Tom Shakespeare, Kath Gillespie-Sells, and Dominic Davies summarize the barriers to sexual liberation in institutions: “Disabled people’s rights to sexual expression, on the one hand, and to freedom from sexual abuse, on the other hand, are not assured in the majority of residential settings.”
Institutions are ill-equipped to deal with the harm of institutional violence due to poor reporting and accountability mechanisms and reliance on the carceral state. For instance, right now, the sole redress for sexual violence only furthers the cycle of institutional violence. As prison abolitionists Mariame Kaba and Eva Nagao write, “We know that protection promised by the state is never divorced from punishment, and that punishment is the glue that keeps patriarchy firmly in place.”
Vicky:
A solution to many of the problems in institutions – violence, harm, and lack of access to sex – is privacy. When my friends come over, I’m embarrassed about where I live, I’m ashamed. Typically, when you go to someone’s house, you knock on their door, and you say, “Hello, can I come in please?” And some of my personal care attendants don’t do that. That can be very awkward for me, especially if, like I said, I’m either in a meeting or a girl’s got needs!
I’ve been subject to more harm and violence in this system than I would ever have been if I were living in the community.
Megan:
Vicky’s experiences of infantilization and desexualization emphasize the importance of what disability theorist Tobin Siebers refers to as the “sexual culture for disabled people.” This can look like disabled people hacking sex toys (Eva Sweeney runs a Cripping Up Toys workshop), mapping erogenous zones (disabled sex educator Kaleigh Trace, author of Hot, Wet & Shaking, does this), or having facilitated or supported sex. The sexual culture of disabled people teaches us the infinite possibilities of sex, beyond heteronormative sexuality and penetration. There is a wide world of disability sex, but institutions close the doors on those possibilities.
Sex is great, but it’s about more than just sex. Movements for reproductive justice must include supporting the sexual lives of people labelled with intellectual/developmental disabilities. Ending institutionalization is a pretty great place to start.